
Occupational Disease@COSHaW
INTRODUCTION
An occupational disease is an illness or health condition that arises as a direct result of a person's work or occupational environment. These conditions are caused by exposure to hazards or substances in the workplace, such as chemicals, radiation, or physical stressors. Examples of occupational diseases include hearing loss due to excessive noise exposure, lung diseases from inhaling harmful substances like asbestos, and musculoskeletal disorders caused by repetitive motion or heavy lifting. Unlike occupational injuries, which usually result from a specific event or accident, occupational diseases may develop gradually over time as a result of prolonged exposure to a hazardous substance or work environment.
Occupational diseases can have serious long-term health consequences and can significantly impact an individual's quality of life. They can also result in lost productivity, increased healthcare costs, and reduced economic growth. As such, it is important for employers to identify and mitigate workplace hazards to prevent occupational diseases from occurring, and for workers to be aware of the risks associated with their job and take appropriate precautions to protect themselves.
OCCUPATIONAL LUNG DISEASE
What is Occupational Lung Disease?
Occupational lung disease refers to lung conditions that develop as a result of exposure to harmful substances in the workplace. These substances can include dust, gases, vapors, fumes, and other airborne particles that can be inhaled into the lungs. Occupational lung diseases happen when workers breathe in certain chemicals, dusts, and fibers that irritate the lungs.These diseases may take a long time to develop. They may have lasting effects on lungs and breathing long after a worker stops working with them.
DIFFERENT TYPES OF OCCUPATIONAL LUNG DISEASE
- OCCUPATIONAL ASTHMA
Occupational asthma is a type of asthma that is caused or exacerbated by exposure to specific substances or conditions in the workplace Asthma is a condition in which your airways narrow and swell and may produce extra mucus. It occurs when you breathe in chemical fumes, gases, dust or other substances on the job.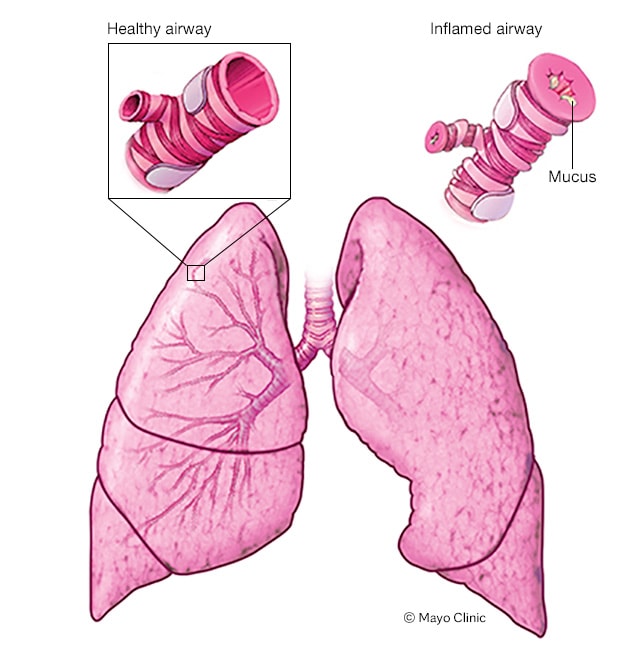
TYPES OF OCCUPATIONAL ASTHMA
- Allergic Occupational Asthma: This type of occupational asthma is triggered by exposure to allergens in the workplace. Workers become sensitized to specific allergens present in their work environment, leading to an allergic immune response and airway inflammation.
- Non-Allergic (Irritant-Induced) Occupational Asthma: In this subtype, exposure to irritants or toxic substances in the workplace can lead to the development of asthma symptoms.Non-allergic occupational asthma does not involve an allergic immune response but direct irritation of the airways.
FACTORS OF EXPOSURE
ALLERGIC OCCUPATIONAL ASTHMA
- Allergens: common allergens might include dust mites, pollen, animal dander, latex proteins, and various proteins or enzymes found in certain occupational settings.
- Irritants: These may include fumes, gases, or particulate matter, such as chemicals, solvents, or strong odors, which can irritate the airways and lead to asthma symptoms.

NON-ALLERGIC OCCUPATIONAL ASTHMA
- Irritants:Common examples include:
- Isocyanates
- Flour and Grain Dust.
- Ammonia:.
- Wood Dust: Sensitizers:
- Sensitizers: Examples include:
- Anhydrides
- Platinum Salts
- Enzymes
WORKERS AT RISK
- Textile Workers.
- Woodworkers
- Hairdressers
- Painters
- Laboratory Workers
RISK FACTOR
- Duration and Intensity of Exposure: Prolonged or high-intensity of exposure to the triggering substances exposure increases the risk.
- Respiratory Protection and Safety Measures: Lack of adequate respiratory protection and safety measures in the workplace can increase the risk.
- Family History: A family history of asthma or allergies may increase an individual's susceptibility to developing occupational asthma.
SYMPTOMS
- Coughing, especially at night or upon waking
- Shortness of breath
- Increased mucus production
- Reduced lung function
- PNEUMOCONIASIS
Pneumoconiosis is a type of lung disease that is caused by the inhalation of various types of mineral dust or other particulate matter over an extended period of time. These dust particles can accumulate in the lungs and cause inflammation and scarring, which can lead to respiratory problems.
WORKER AT RISK
- Coal Miners
- Glass Manufacturing Workers
- Construction Workers
- Ceramic and Pottery Workers

Glass Manufacturing workers. Coal Miners.
TYPES OF PNEUMOCONIASIS
I. ASBESTOSIS
Asbestosis is caused by the inhalation of asbestos fibers, commonly found in construction materials, insulation, and various industrial applications. Over time, asbestos fibers can lead to lung fibrosis and impaired lung function and lead to cancer.
FACTORS OF EXPOSURE
- Occupational Exposure: Workers in certain industries, such as construction, asbestos mining,and manufacturing, are at a higher risk of inhaling asbestos fibers.
- Direct Inhalation of Asbestos Fibers: Asbestosis develops when individuals inhale asbestos fibers, cause inflammation.
- Secondary Exposure: Family members of asbestos workers can be at risk of secondary exposure to asbestos fibers brought home on clothing, skin, or hair.
RISK FACTORS
- Duration and Intensity of Exposure: Prolonged or high-intensity of exposure asbestos increases the risk.
- Age: Older individuals who were exposed to asbestos earlier in their careers may have a higher risk of developing asbestosis.
- Lack of Protective Measures: Failure to use appropriate personal protective equipment (PPE), such as respirators and protective clothing increases the risk.
SYMPTOMS
- Shortness of Breath
- Persistent dry Cough
- Chest Tightness or Pain
- Fatigue

II. SILICOSIS
Caused by breathing in tiny bits of silica, a mineral found in sand, quartz, and many other types of rock.Silicosis mainly affects workers exposed to silica dust in mining, paint manufacturing, glass and concrete product manufacturing, foundries, brick making, construction, and manufacturing of plumbing fixtures.
FACTORS OF EXPOSURE
-
- Inhalation of Silica Dust: Silicosis occurs when individuals inhale respirable crystalline silica dust, which consists of tiny airborne particles of crystalline silica.
- Size of Silica Particles: These small particles are more likely to reach the deepest parts of the lungs, where they can cause damage.
- Secondary Exposure: Family members or others in close contact with workers bring home silica dust on their clothing and skin.
RISK FACTORS
- Occupational Exposure: Industries where workers are at risk include construction, foundries, and certain types of manufacturing (e.g., ceramics and concrete).
- Duration and Intensity of Exposure: Prolonged and high-intensity exposure increases the likelihood of developing the disease.
- Poor Ventilation: Workplaces with inadequate ventilation systems can result in the accumulation of silica dust in the air,increasing the risk of exposure.
SYMPTOMS
- Shortness of Breath
- Persistent dry Cough
- Chest Tightness or Pain
- Fatigue

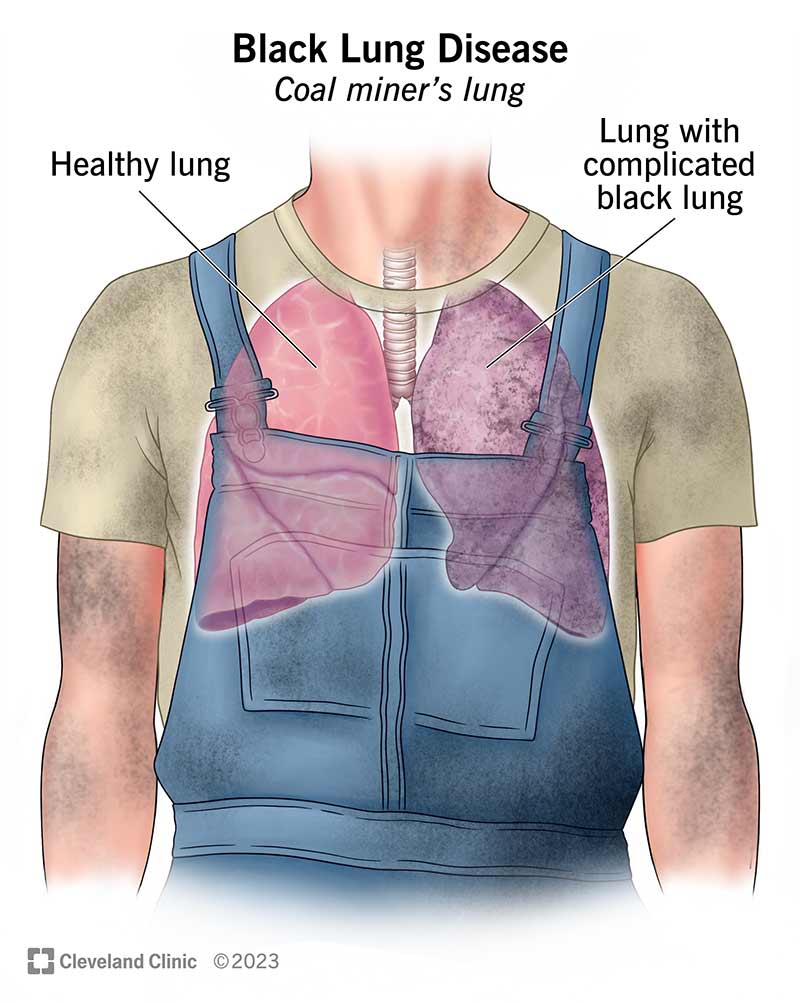
III. COAL WORKER'S PNEUMOCONIASIS
Coal Workers' Pneumoconiosis (CWP), commonly referred to as "black lung disease," is an occupational lung disease related to the inhalation of coal dust over an extended period of time in coal mining and related industries.
FACTORS OF EXPOSURE
- Inhalation of Coal Dust: Coal Worker's Pneumoconiosis develops when individuals inhale fine coal dust particles that are released into the air during coal mining and related activities.
- Coal Dust Accumulation: Over time, inhaled coal dust particles accumulate in the lungs.The body's natural defense mechanisms are unable to remove these particles effectively.
RISK FACTORS
- Duration of Exposure:Prolonged of exposure to coal dust increases the risk developing Coal Worker's Pneumoconiasis (CWP).
- Occupational Exposure to Coal Dust: Miners who work in underground coal mines or in areas with high levels of coal dust are at the highest risk.
- Intensity of Exposure: Workers exposed to high levels of coal dust concentration are at a greater risk of developing CWP.
SYMPTOMS
- Coughing up Black Sputum
- Wheezing
- Shortness of Breath
TREATMENT
OCCUPATIONAL ASTHMA
Depending on the type of medicine, you may breathe in the drugs or take them by mouth. A metered-dose inhaler,nebulizer or other inhaler delivers some medication when you breathe it.
PNEUMOCONIASIS
- Medications:These may include bronchodilators to improve airflow, cough suppressants, and medications to reduce inflammation.
- Oxygen Therapy: In cases where pneumoconiosis has significantly impaired lung function and oxygen levels are low, oxygen therapy may be prescribed to improve oxygenation.
- Vaccinations: Patients with pneumoconiosis are often encouraged to receive vaccinations against respiratory infections like influenza and pneumonia to reduce the risk of complications.
PREVENTION AND MANAGEMENT
Individual strategies
- Work with your employer if you are still in the same position to ensure access to the appropriate protective equipment.
- Attend repeated safety trainings on how to minimize your exposure to harmful substances in the workplace.
- Reduce your exposure to lung irritants outside of work. Don't smoke or vape and avoid secondhand smoke and aerosol whenever possible.
- Safety policies:All businesses whose workers handle common irritants should develop policies to protect employees.
- Proper ventilation:Employers should install appropriate ventilation to remove irritants and circulate fresh air.
- Substitutions for hazardous materials: If possible, companies should find lower-risk alternatives.

REFERENCES
- Pneumoconiosis. Johns Hopkins Medicine. (2019, November 19). https://www.hopkinsmedicine.org/health/conditions-and-diseases/pneumoconiosis#:~:text=Pneumoconiosis%20is%20one%20of%20a,usually%20take%20years%20to%20develop.
- Association, A. L. (n.d.). Occupational lung disease. Occupational Lung Disease | American Lung Association. https://www.lung.org/lung-health-diseases/lung-disease-lookup/occupational-lung-diseases#:~:text=Tobacco%20smoke%20is%20a%20leading,construction%2C%20transportation%20or%20healthcare%20support.(Occupational Lung Disease, n.d.)
- Government of Canada, C. C. for O. H. and S. (2023, June 13). Asthma, work-related. https://www.ccohs.ca/oshanswers/diseases/asthma.html
- Source of video below: Occupational lung diseases in the manufacturing industry. YouTube. (2021, June 17). https://youtu.be/6HPSqYo5yBs?feature=shared
OCCUPATIONAL SKIN DISEASE
What is Occupational Skin Disease?
Occupational skin disease (OSD) is a type of occupational disease that affects the skin. Occupational skin disease is among the most common occupational diseases reported. For a skin disease to be considered occupational in origin, there must be a causal relationship between the occupation or work and the skin disease.There are three broad groups of occupational skin disease:
- Irritant contact dermatitis
- Allergic contact dermatitis
- Another occupational skin disease

FACTORS OF EXPOSURE
Occupational skin disease may follow exposure to chemical, biological or physical agents.
Chemical exposure
- Numerous chemicals including rubber additives, hair dyes, preservatives, epoxy resins and acrylates can cause contact allergic dermatitis.
- Tar and arsenic have been associated with skin cancer.
- Cement under occlusion can cause a chemical burn.
Biological exposure
- Contact with animals may result in infections such as orf (from sheep and goats), milker’s nodules (from cows) and tinea corporis / ringworm (from horses, cattle, pigs, cats and dogs).
- Contact with infected/infested humans may result in infections such as impetigo and tinea corporis /ringworm and infestations such as scabies and head lice.
- Contact with insects may result in contact urticaria from caterpillars and cockroaches, and arthropod-borne viral skin infections or protozoa infections.
- Contact with plants may result in urticaria from nettles, and allergic contact plant dermatitis from sap from cut stems of daffodils, dahlias, chrysanthemums, and Peruvian lilies and wood resins.
Physical exposure
- Mechanical trauma to the skin leads to cuts, blisters, calluses, blood clots, and basal cell carcinoma may arise in thermal burn and other scars.
- Direct heat causes thermal burns.
- Hot humid environments may provoke acne, sweat rash (miliaria), intertrigo (chafing), skin maceration and supervening bacterial infection or fungal infection. Low humidity environments may result in chapping and fissures and cold environments cause frostbite, chilblains, cold urticaria, Raynaud phenomenon.
- Ultraviolet radiation is the main cause of skin cancer and photoaging.
- Ionizing radiation (X-rays, α, β, and γ rays) may cause radiation dermatitis and radiation-induced skin cancer.
- Physical irritants such as particulates, rough surfaces, and fibers (eg fiberglass) may cause irritant dermatitis.
WORKERS AT RISK
The following occupations account for 80% of reported occupational skin disease in developed countries in Europe; most involve wet working conditions, which commonly results in contact dermatitis.
- Hairdressing/ beauty therapy
- Food industry
- Health care including dental and veterinary workers
- Laboratory workers, including scientists and laboratory technicians
- Agriculture including farmers, gardeners and florists
- Cleaning
- Painting and decorating
- Motor vehicle repair
- Construction work
- Printing
- Homemakers
Younger workers have a slightly higher risk that older workers, but who are affected will depend on:
- Individual predisposition – particularly atopic dermatitis/eczema or sensitive skin
- Personal hygiene
- Circumstances of exposure.
|
TYPES |
SYMPTOMS |
EXPOSURE |
|
Irritant contact dermatitis Irritant contact dermatitis is a form of skin inflammation caused by contact with substances and/or environmental factors that injure the skin, damaging the skin barrier.
|
·Usually is confined to the site of contact with the irritant ·Burning and pain more common symptoms than itch ·Acute due to a single severe exposure ·Localised well-defined, redness, papules, swelling, blistering (vesicles/bullae) ·Example: kneeling in wet cement, which is very alkaline, causing severe dermatitis of the knees ·Chronic due to mild irritants or repetitive cumulative exposure ·Initial dryness and cracking of the skin ·Evolves to include inflammatory changes with redness and itch ·May develop tolerance or hardening with time ·Examples include dribble rash, napkin dermatitis, housewife’s eczema, Interdigital dermatitis, also called the ‘sentinel sign’, is regarded as an early stage of irritant contact dermatitis affecting the hands. It is commonly seen in occupations involving wet work.
|
- Occupational hand dermatitis is due to irritants in 80% of cases, most often affecting those who involved in wet work such as cleaners, hairdressers, food handlers, and healthcare personnel. Irritant contact dermatitis can affect all age groups, both sexes, and any race.
- Occupational irritants can include wet work, detergents, solvents, acids, alkalis, adhesives, and metalworking fluids. - Topical medications such as retinoids and benzoyl peroxide, may cause irritant contact dermatitis with long-term use. - Friction, sweating, and heat are examples of environmental factors. - Irritant dermatitis is often the result of the cumulative impact of multiple irritants. |
|
Allergic contact dermatitis Allergic contact dermatitis is a form of dermatitis/eczema caused by an allergic reaction to a material, called an allergen, in contact with the skin. The allergen is harmless to people that are not allergic to it. Allergic contact dermatitis is also called contact allergy
Adhesive plaster reaction |
Allergic contact dermatitis arises some hours after contact with the responsible material. It settles down over some days providing the skin is no longer in contact with the allergen.
Allergic contact dermatitis is generally confined to the site of contact with the allergen, but it may extend outside the contact area or become generalised. ·Transmission from the fingers can lead to dermatitis on the eyelids and genitals. ·Dermatitis is unlikely to be due to a specific allergen if the area of skin most in contact with that allergen is unaffected.
Some typical examples of allergic contact dermatitis include: ·Eczema in the skin in contact with jewellery items, due to contact allergy to nickel ·Eczema under adhesive plaster, due to contact allergy to rosin ·Swelling and blistering of face and neck in reaction to permanent hair dye, due to allergy to paraphenylenediamine ·Hand dermatitis caused by rubber accelerator chemicals used in the manufacture of rubber gloves
There is a very long list of materials that have caused contact allergy in a small number of individuals. |
- Allergic contact dermatitis is especially common in metal workers, hairdressers, beauticians, health care workers, cleaners, painters, and florists.
- It is more common in women than men, mainly due to nickel allergy and, recently, to acrylate allergy associated with nail cosmetics. - Many young children are also allergic to nickel. - Contact allergy to topical antibiotics is common in patients over the age of 70 years old.
|
|
Urticaria Contact urticaria is an immediate but transient localised swelling and redness that occurs on the skin after direct contact with an offending substance. Contact urticaria should be distinguished from contact dermatitis where a dermatitis reaction develops hours to days after contact with the offending agent.
Contact urticaria can be immunological (due to allergy) or non-immunological. It is a form of inducible urticaria and can be acute or chronic.
|
Contact urticaria reactions appear within minutes to about one hour after exposure of the offending substance to the skin. Signs and symptoms of affected skin areas include: ·Local burning sensation, tingling or itching ·Localised or generalised red swellings or weals may occur, especially on the hands. ·Rash usually resolves by itself within 24 hours of onset.
Signs and symptoms may occur in other organs other than the skin. These are known as extracutaneous reactions and are more likely to occur in patients with immunological contact urticaria. Features of extracutaneous reactions include: ·Wheezing (bronchial asthma) ·A runny nose, watery eyes ·Lip swelling, hoarse throat, difficulty swallowing ·Nausea, vomiting, diarrhoea, cramps ·Severe anaphylactic shock (this can be life-threatening)
|
Occupational groups at risk and the substances that cause contact urticaria are listed below. ·Agricultural and dairy workers: cow dander, grains and feeds ·Bakers: ammonia persulfate, flour, alpha-amylase ·Dental workers: latex, acrylate and epoxy resins, toothpaste ·Electronic workers: acrylate and latex ·Food workers: foodstuffs, such as cheese, egg, milk, fish, shellfish, fruit, flour, wheat ·Hairdressers: ammonia persulfate, latex ·Medical/veterinary workers: latex
|
|
Skin cancer Skin cancers are malignant tumours in which there is an uncontrolled proliferation of any one of the many skin cell types, whereas the normal process of regeneration of skin involves replication of the cells in a controlled fashion. Each subtype of skin cancer has unique characteristics.
The most common forms of skin cancer are: ·Basal cell carcinoma (BCC) ·Squamous cell carcinoma (SCC), including keratoacanthoma ·Melanoma. The term non-melanoma skin cancer refers to all types of skin cancer apart from melanoma. BCC and SCC are also called keratinocyte cancer.
|
Skin cancers generally appear as a progressive lump or nodule, an ulcer, or a changing lesion. Signs of advanced, aggressive, or neglected skin cancer may include: ·Ulceration ·Bleeding ·Local invasion and destruction of adjacent tissues and structures ·Distant spread of a tumour to lymph glands and other organs such as liver and brain (metastasis).
|
Skin cancer most commonly affects older adults, but it can also affect younger adults, and rarely, children. Most often affect those who are construction workers, agriculture workers, firefighters, police officers and defence workers, airline workers, and any outdoor workers.
The common forms of skin cancer listed above are related to exposure to ultraviolet radiation (from sunlight or tanning beds) and the effects of ageing. Other risks include:
|


:max_bytes(150000):strip_icc()/VWH_DermNet_Allergic-Contact-Dermatitis-Plaster_01-04427e0f167644aaa9a8d8a4efd2e8e5.jpg)






TREATMENT
For therapeutic purposes, contact dermatitis can be classified as acute or chronic. Therapeutic measures can almost always provide some relief, but cure depends on identification of the offending agent and cessation of exposure.
- ACUTE DERMATITIS
- Wet Dressings
- Steroids
- Systemic Antihistamines
Diphenhydramine (e.g., Benadryl), in a dosage of 25 to 50 mg three or four times daily, or hydroxyzine hydrochloride (Atarax), in a dosage of 25 mg three or four times daily, provides an antipruritic effect. Doxepin (Sinequan), in a dosage of one to three 10-mg capsules taken at night as needed, is effective, but patients should be monitored for anti-cholinergic effects. A 5 percent doxepin cream (Zonalon) is also effective.
2. CHRONIC DERMATITIS
- Emollients
Topical agents such as petrolatum (Vaseline) provide an occlusive film over inflamed skin, decrease fissuring, and reduce evaporation. Emollients are most effective when they are applied after skin has been soaked or washed in water.
- Topical Steroids
Treatment with higher potency fluorinated steroids, such as 0.05 percent fluocinonide (Lidex), in contrast to mid-potency 0.1 percent triamcinolone acetonide (Kenalog), is indicated in patients with more persistent dermatitis or chronic dermatitis affecting the hands. Occlusion with plastic wrap or plastic gloves enhances absorption.

PREVENTION AND MANAGEMENT
Individual strategies
- Employers and workers should be involved in identifying workplace hazards.
- Skin contact with the hazard can be avoided by using encapsulated machines or automated equipment, such as dishwashers and food mixer.
- Use personal protective equipment: gloves, aprons, face shields.
- Optimise skin barrier function with suitable emollients, barrier and moisturising creams.
- Topical or oral steroids, emollients, and antibiotics should be prescribed as indicated by a medical professional
Workplace initiatives
- Evaluate the exposure to hazards, and assess the risk of harm.
- Maintain a register of accidents/incidents/occupational disease.
- Where possible, choose less harmful chemicals to do the same job.
- Rotate tasks to reduce individual exposure
- Provide safety data sheets.
- Train workers on causes of occupational skin disease.
- Train workers how to protect their skin from injury and dermatitis.
- Move at-risk individuals to alternative work.
- Where a hazard is minimised, monitor workers’ health with respect to that hazard.

REFERENCES
- Occupational skin disease. DermNet. (n.d.). https://dermnetnz.org/topics/occupational-skin-disease
- Diseases and conditions. American Academy of Dermatology. (n.d.). https://www.aad.org/public/diseases/
- World Health Organization. (n.d.-b). Occupational Health: Health Workers. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/occupational-health--health-workers
- NHS. (n.d.). NHS choices. https://www.nhs.uk/conditions/
- Source of video below: Occupational skin diseases. YouTube. (2018, March 19). https://youtu.be/sXrWDM8-1xY?feature=shared
OCCUPATIONAL NEUROTOXICITY
Occupational Neurotoxicity refers to the harmful effects that contain chemicals or toxins in the workplace which can affect on the nervous system. This can include damage to the brain, spinal cord, and peripheral nerves. Some common chemicals that can cause occupational neurotoxicity include lead, mercury, organic solvents (such as benzene and toluene), pesticides, and certain metals like manganese and aluminum. This can occur when the normal functioning of the nervous system is altered by exposure to harmful substances (neurotoxicants). Neurons (nerve cells),which are crucial for transmitting and processing signals in the brain and other parts of the nervous system, may eventually become disrupted or even killed as a result of this.


FACTORS OF EXPOSURE
- Lead
- Mercury
- Insecticides
- Industrial and cleaning solvents
- Car exhaust
- Chlorine
- Formaldehyde
- Chemotherapy drugs
- Heavy metals such as mercury and lead
- Cosmetics
- Drug therapies
- Radiation
- Certain foods and food additives
 Mercury
Mercury
WORKERS AT RISK
Workers in industries such as:
- Chemical manufacturing and handling: Workers involved in chemical plants, laboratories, and facilities involved in pesticide production.
- Construction and demolition: Workers exposed to lead, solvents, or asbestos during painting, sanding or demolition.
- Healthcare and laboratories: Workers who are working with certain drugs, anesthetic gases, or diagnostic agents.
- Plastics manufacturing: Some plastic production processes involve the use of neurotoxic chemicals.
- Agriculture and pesticide application: Farmers who are exposed to neurotoxic pesticides, herbicides and insecticides.
- Manufacturing and use of metals: Workers who are exposed to heavy metals like lead, mercury or manganese
RISK FACTORS
- Exposure to toxic chemicals: Workers who are exposed to certain chemicals such as lead, mercury, pesticides, and organic solvents are at increased risk of neurotoxicity.
- Duration of exposure: The longer a worker is exposed to a toxic chemical, the greater the risk of developing neurotoxicity.
- Concentration of exposure: Workers who are exposed to high concentrations of toxic chemicals are at greater risk of developing neurotoxicity than those who are exposed to lower concentrations.
- Route of exposure: Inhalation and skin contact are the most common routes of exposure in the workplace.
- Age and health status: Older workers and those with pre-existing medical conditions such as diabetes or hypertension may be more susceptible to develop neurotoxicity
- Genetic susceptibility: Certain genetic factors can make individuals more susceptible to the effects of neurotoxic chemicals.
- Lifestyle factors: Lifestyle factors such as smoking and alcohol consumption can also increase the risk of neurotoxicity.
SYMPTOMS
- Headaches
- Dizziness & vertigo
- Fatigue
- Irritability & mood changes
- Memory loss & confusion
- Tremors and shaking
- Muscle weakness & loss of coordination
- Tingling or numbness in the extremities
- Vision and hearing problems
- Seizures or convulsions
TREATMENT
- Immediate care
- Removal from exposure
- Supportive care
- Monitoring
- Symptomatic relief
- Decontamination
- Specific antidotes
- Chelation therapy
- Respiratory support
- Neurological interventions
- Antiseizure medications (Phenytoin, Carbamazepine, Valproic acid, Gabapentin, Ethosuximide)
- Neuroprotective agents (Omega-3 fatty acids, melatonin, erythropoietin)
- Rehabilitation and supportive therapy
- Psychological support
- Follow-up care
PREVENTION & MANAGEMENT
Individual strategies
- Proper Handling and Storage
- Follow recommended procedures for the handling, storage, and disposal of hazardous materials. This helps minimize the risk of exposure.
- Good Hygiene Practices
- Wash your hands thoroughly after handling chemicals or materials that may be neurotoxic. Avoid touching your face, eyes, nose, or mouth while working.
- Regular Health Check-ups
- Attend regular medical check-ups and screenings, especially if you work in an environment where you are exposed to neurotoxic substances.
- Adequate Nutrition and Hydration
- Maintain a healthy diet and stay hydrated. Proper nutrition can support overall health, including the nervous system.
- Substitution and Engineering Controls
- Prioritize the use of less hazardous substances or engineering controls to minimize exposure. This may include replacing neurotoxic chemicals with safer alternatives or implementing closed systems for handling hazardous materials.
- Safe Work Practices and Standard Operating Procedures (SOPs):
- Develop and enforce SOPs for handling, storing, and disposing of neurotoxic substances. Ensure that all employees are trained on these procedures.
- Training and Education
- Provide comprehensive training to employees about the hazards associated with neurotoxic substances, as well as safe work practices and emergency response procedures.
- Emergency Response and First Aid
- Develop and communicate clear procedures for responding to spills, leaks, or accidental exposures to neurotoxic substances. Ensure that appropriate first aid measures are readily available.
REFERENCES
- U.S. Department of Health and Human Services. (n.d.). Neurotoxicity. National Institute of Neurological Disorders and Stroke. https://www.ninds.nih.gov/health-information/disorders/neurotoxicity
- Robertson, S. (2022, December 31). What is neurotoxicity?. News. https://www.news-medical.net/health/What-is-Neurotoxicity.aspx
- Laboratory safety guidance - occupational safety and health administration. (n.d.). https://www.osha.gov/sites/default/files/publications/OSHA3404laboratory-safety-guidance.pdf
- Chemical hazards and toxic substances - overview. Occupational Safety and Health Administration. (n.d.). https://www.osha.gov/chemical-hazards
- Source of video below: Lead poisoning symptoms, causes, treatment. YouTube. (2022, February 3). https://youtu.be/ukRbasguAFY?feature=shared
OCCUPATIONAL MUSCULOSKELETAL DISORDERS
What is Occupational musculoskeletal disorders?
Musculoskeletal disorders (MSD) are conditions that affect your muscles, nerves, tendons, joints, cartilage, and spinal discs. When these conditions are linked to workplace factors, they are termed "occupational MSDs”. They can cause pain and discomfort, making it essential to understand the role of your work environment in these conditions.
Examples of MSDs Include:
- Sprains, strains, and tears
- Back pain
- Carpal tunnel syndrome

WORKERS AT RISK
- Healthcare workers
- Firefighters and prevention workers
- Laborers and freight, stock and material movers
- Janitors and cleaners
- Heavy and tractor-trailer truck drivers
- Maids and housekeeping cleaners
- Light truck or delivery services drivers
- Telecommunications line installers and repairers
- Bus drivers, transit and intercity
- Production workers
- Police and sheriff patrol officers
- Heating, air conditioning, and refrigeration mechanics and installers
- Plumbers, pipefitters and steamfitters
- Maintenance and repair workers, general



RISK FACTORS
-
Certain work conditions can lead to MSD. These conditions include:
- Routine lifting of heavy objects.
- Daily exposure to whole-body vibration.
- Routine overhead work.
- Maintaining your neck in a chronic flexed position.
- Performing repetitive and forceful tasks.
SYMPTOMS
-
Occupational Musculoskeletal Disorders (MSDs) often present with pain as the most common symptom. Workers experiencing MSDs may also notice other symptoms, such as:
- Joint Stiffness: A feeling of reduced mobility in affected joints.
- Muscle Tightness:Muscles may feel tense and inflexible.
- Redness and Swelling:The affected area may become red and swollen.
- "Pins and Needles" Sensations: Numbness and tingling, similar to pins and needles, in the affected area.
- Numbness: A loss of sensation in the affected region.
- Skin Color Changes: Skin discoloration may occur.
- Decreased Sweating of the Hands: Reduced sweat production in the hands.
Responding promptly by seeking medical attention and adjusting work practices can help prevent the progression of MSDs and promote a quicker recovery. Listening to your body and addressing symptoms promptly is key to managing and preventing MSDs.


TREATMENT
Occupational Musculoskeletal Disorders (MSDs) require a variety of treatment approaches. Here's how they can be treated:
- Restriction of Movement
- Limiting activities that worsen the condition. Sometimes, this means changing your work tasks or responsibilities to avoid further strain. Redesigning the job to prevent excessive strain on the joints is often a better solution.
- Application of Heat or Cold
- Heat and cold therapy can help relieve pain and speed up the healing process. Cold therapy is useful for reducing pain and swelling in injuries or inflamed areas, while heat therapy can alleviate muscle pain by increasing blood flow.
- Exercise
- Stretching and exercise can be beneficial as they improve circulation and reduce muscle tension. However, individuals with WMSDs should consult a physical therapist before starting any exercise program.
- Medication and Surgery
- Anti-inflammatory medications can help reduce pain and inflammation associated with WMSDs. If other treatments don't provide relief, a healthcare professional might consider more advanced treatments or, in severe cases, surgery.
PREVENTION & MANAGEMENT
Individual strategies
- Use Proper Techniques
- Always use proper lifting and handling techniques to avoid unnecessary strain on your muscles and joints.
- Worker Involvement
- Workers can help by identifying workplace hazards, providing input during assessments, and evaluating changes resulting from ergonomic improvements.
- Encourage Early Reporting of MSD symptoms
- It speeds up the assessment and improvement process, reducing the risk of severe injuries and lost-time claims.
- Use of personal protective equipment
- For example, items like braces, wrist splints, and back belts may reduce the duration, frequency, or intensity of exposure in some situations.
- Provide Management Support
- Management should set clear goals, communicate them with workers, assign responsibilities to staff members, and maintain open communication.
- Provide Training
- Training ensures that workers understand ergonomics, its benefits, and how to address ergonomic concerns in the workplace.
- Identify Problems
- Early identification of ergonomic issues in the workplace is crucial to prevent MSDs from occurring.
- Control or eliminate workplace MSD hazards
- These solutions may include changes in equipment, workstations, or procedures.
REFERENCES
- Work-Related Musculoskeletal Disorders & Ergonomics. (2023). https://www.cdc.gov/workplacehealthpromotion/health-strategies/musculoskeletal-disorders/index.html
- Ergonomics - Overview | Occupational Safety and Health Administration. (2013). Osha.gov. https://www.osha.gov/ergonomics
- Which workers are at highest risk of MSDs? (2018, November 8). Ishn.com; ISHN. https://www.ishn.com/articles/109750-which-workers-are-at-highest-risk-of-msds
- Canada,. (2014). Work-related Musculoskeletal Disorders (WMSDs). Ccohs.ca. https://www.ccohs.ca/oshanswers/diseases/rmirsi.html
- Source of video below: Musculoskeletal disorders – an introduction. YouTube. (2021a, August 9). https://youtu.be/7ib0lCAP8yw?feature=shared
NOICE-INDUCED HEARING LOSS
What is Noice-Induced Hearing Loss?
Noise-induced hearing loss is a type of hearing impairment that can be temporary or permanent, and it can affect one ear or both ears.Jobs that involve machinery, equipment, tools, or processes that generate high levels of noise are at a higher risk of causing NIHL.NIHL is one of the most common occupational diseases worldwide. It can affect workers in various industries and occupations.

RISK FACTORS
1. Noise Level: Sounds above a certain decibel level (typically around 85 decibels or higher) can cause damage with prolonged exposure.2. Duration of Exposure: The longer a person is exposed to loud noises, the greater the risk of hearing damage. Short, intense bursts of noise can also be harmful, but sustained exposure over time is a significant risk factor.
3. Lack of Hearing Protection: Failure to use appropriate hearing protection devices, such as earplugs or earmuffs increase the risk of NIHL.

WORKERS AT RISK
-
Manufacturing and Industrial Workers:
- Factory workers
- Machine operators
- Metalworkers
-
Transportation Workers:
- Airport ground crew
- Aircraft maintenance personnel
- Truck drivers
-
Construction and Mining Workers:
- Construction site workers
- Quarry workers
- Drillers

SYMPTOMS
- Reduce hearing in one or both ear
- Ringing or buzzing sound, which is also called ‘tinnitus’
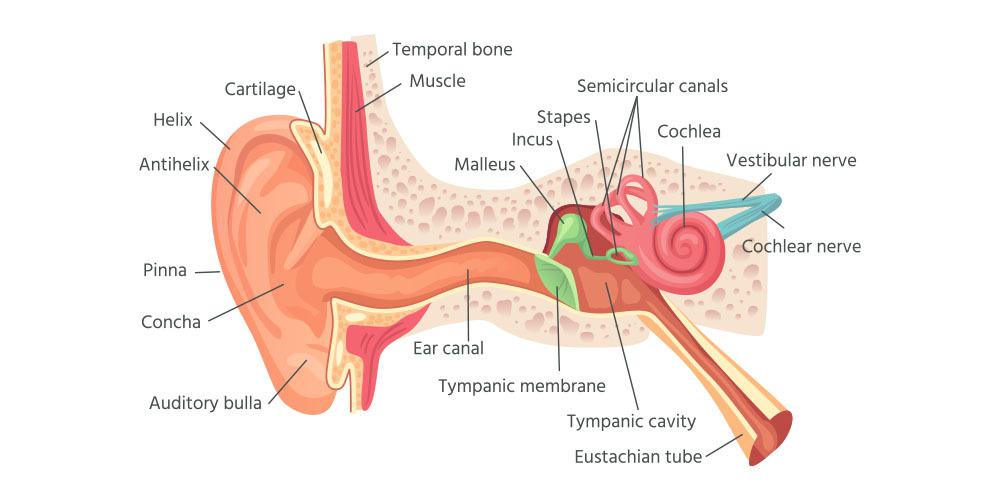
It is a permanent condition since the nerve in the cochlea has been damaged. The nerve cannot regrow. The ear normally does not show any physical changes. There will be no ear discharge and the eardrum looks normal as well.
TREATMENT
- Seek further treatment from Ear, Nose & Throat (ENT) Specialist
- Perform an audiometry test if you are having the symptom. It is a special test to confirm that you have hearing loss.
- Treatment options for hearing loss : hearing aid and surgery
- If you have noise induced hearing loss report to the employer
PREVENTION AND MANAGEMENT
- Avoid or limit exposure to excessively loud sounds
- Move away from the source of loud sounds when possible
- Use hearing protection devices when it is not feasible to avoid exposure to loud sounds or reduce them to a safe level such as ear plug/ear muff.
Workplace initiatives
- Choose low-noise tools and machinery
- Maintain and lubricate machinery and equipment
- Place a barrier between the noise source and employee (e.g., sound walls or curtains).
- Enclose or isolate the noise source.
- Operating noisy machines during shifts when fewer people are exposed.

REFERENCES
- Wikimedia Foundation. (2023, October 14). Noise-induced hearing loss. Wikipedia. https://en.wikipedia.org/wiki/Noise-induced_hearing_loss
- From the Institute for Medical Sociology. (n.d.). Exploring the association between Social Capital and... : Journal of Occupational and Environmental Medicine. LWW. https://journals.lww.com/joem/fulltext/2012/01000/exploring_the_association_between_social_capital.8.aspx
- Source of video below: Explained - how excessive loud noise is damaging your ears. YouTube. (2019, January 14). https://youtu.be/ZS9YYj-Ad4U?feature=shared
OCCUPATIONAL MENTAL ILLNESS
What is Occupational Mental Illness?
Occupational Mental Illness refers to mental health conditions or disorders that are directly or indirectly caused or exacerbated by factors related to a person's work or employment. These conditions can result from various workplace-related stressors, such as high job demands, low job control, long working hours, bullying or harassment, and exposure to traumatic events.
Occupational mental illnesses can encompass a wide range of disorders, including but not limited to:
- Stress-related disorders
- Acute stress disorder or post-traumatic stress disorder (PTSD), which can be triggered by traumatic incidents or prolonged exposure to stressful work conditions.
- Depressive disorders
- Major depressive disorder, which may be influenced by chronic work-related stress, feelings of inadequacy, or a hostile work environment.
- Anxiety disorders
- Generalized anxiety disorder or panic disorder, which can be exacerbated by high-pressure work environments, excessive job demands, or a lack of control over work-related situations.
- Burnout
- A state of chronic physical and emotional exhaustion often linked to prolonged exposure to demanding or emotionally draining work environments.
- Substance abuse disorders
- Some individuals may turn to substance abuse as a way to cope with workplace stress or other mental health challenges.
- Sleep disorders
- Irregular working hours, high job demands and stress can contribute to sleep disorders like insomnia or sleep apnea.
- Adjustment disorders
- These can occur when an individual has difficulty coping with significant changes or stressors in their work environment.
 Substance abuse disorder
Substance abuse disorder
RISK FACTORS
- High job demands: Excessive workload, tight deadlines, and high expectations can contribute to chronic stress and anxiety.
- Lack of control or autonomy: Limited decision-making power or control over one's work can lead to feelings of frustration and helplessness.
- Poor work-life balance: Long or irregular working hours, including overtime and shift work, can disrupt personal life and lead to burnout.
- Job insecurity: Fear of job loss, unstable employment, or frequent reorganization within the company can create chronic stress.
- Workplace bullying or harassment: Hostile or toxic work environments can lead to anxiety, depression and other mental health issues.
- Lack of social support: Feeling isolated or unsupported by colleagues, supervisors, or the organization can contribute to mental health changes.
- Organizational change or restructuring: Uncertainty and upheaval resulting from mergers, layoffs, or major changes in company structure can be stressful.
- Traumatic events: Exposure to accidents, violence, or other traumatic incidents at the workplace can lead to conditions like PTSD.
- Physical health and safety risks: Working in environments with potential physical hazards or high levels of stress due to safety concerns can impact mental well-being.
- Discrimination and inequality: Discrimination based on factors such as race, gender, age, or disability can contribute to mental health changes.
- Inadequate training or resources: Insufficient training or resources to perform job duties effectively can lead to feelings of incompetence and stress.
- Lack of job security or advancement opportunities: A perceived lack of prospects for career growth or development can lead to feelings of stagnation and frustration.
- Organizational culture: A culture that does not prioritize employee well-being, or that fosters competition or hostility, can contribute to mental health issues.
- Work-related travel or commuting stress: Long commutes or extensive travel requirements can lead to fatigue and stress.
SYMPTOMS
- Changes in mood and behaviour
- Persistent feelings of sadness, hopelessness, or irritability
- Social withdrawal or avoidance of colleagues and work-related activities
- Physical symptoms
- Headaches or stomachaches
- Changes in appetite
- Sleep disturbances
- Cognitive difficulties
- Difficulty concentrating, making decisions or remembering tasks
- Emotional instability
- Frequent mood swings
- Increase anxiety
- Decreased work performance
- Excessive work-related thoughts
- Loss of interest or enthusiasm
- Social and relationship challenges
- Strained relationships with colleagues, supervisors or family members due to work-related stressors
- Increased substance use or abuse
- Greater reliance on alcohol, drugs or other substances
- Physical tension or discomfort
- Muscle tension, clenched jaw, or other physical signs of stress or anxiety
- Suicidal thoughts or behaviours
- Thoughts of self-harm or suicide
TREATMENT
- Psychotherapy
- Medication
- Antidepressants (Fluoxetine, Duloxetine, Amitriptyline, Phenelzine)
- Antipsychotics (Haloperidol, Chlorpromazine, Clozapine)
- Anxiolytics (Benzodiazepines)
- Mood stabilizers
- Self-care and lifestyle changes
- Regular exercise
- Balanced nutrition
- Mindfulness and meditation
- Therapeutic activities
- Art therapy
- Music therapy
PREVENTION & MANAGEMENT
Individual strategies
- Self-care practices
- Prioritize regular exercise, balanced nutrition and adequate sleep
- Doing relaxation techniques like deep breathing, mindfulness
- Pursue hobbies and activities that bring joy
- Seek social support
- Effective time management
- Regular health check-ups
Workplace initiatives
- Promote a supportive work environment
- Encourage work-life balance
- Offer mental health resources
- Adress workplace stressors
- Identify and mitigate specific sources of stress in the workplace, such as excessive workload, unrealistic deadlines, or inadequate resources
- Adress workplace bullying and harassment
- Implement clear policies and procedures for reporting and addressing instances of workplace bullying or harassment
REFERENCES
- World Health Organization. (n.d.). Mental health at work. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/mental-health-at-work
- Harvey SB;Modini M;Joyce S;Milligan-Saville JS;Tan L;Mykletun A;Bryant RA;Christensen H;Mitchell PB; (n.d.). Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occupational and environmental medicine. https://pubmed.ncbi.nlm.nih.gov/28108676/
- Mental health and stress in the workplace - centers for disease control ... (n.d.-b). https://www.cdc.gov/workplacehealthpromotion/tools-resources/pdfs/WHRC-Mental-Health-and-Stress-in-the-Workplac-Issue-Brief-H.pdf
- Source of video below: Mental illness causes, symptoms, diagnosis, and treatment: Merck Manual Consumer Version. YouTube. (2020, August 24). https://youtu.be/-squqwaTuxo?si=bsYW-JBdiqkSFVOm
Prepared by Group 17 Pre Clinical Elective Group 2022
Faculty of Medicine, UiTM
AINUN NAJWA BINTI ALIAS (2021816858)
SITI NURSYAHIRAH BINTI SHEIKH NEHMIL EMIR (2021817052)
NURUL NABILAH BINTI KHAIRUN NAWAL (2021823378)
NIK NUR FARHANA BINTI NIK MOHAMED AZHAR (2021823392)
PROF. DR. SITI MUNIRA BINTI YASIN (Main Supervisor)
DR. KAMARULZAMAN BIN MUZAINI (Co-supervisor)
ENCIK MOHD SUPIAN BIN HASSAN (Pharmaniaga Logistics Sdn Bhd)
TC. NUR AIMAN BIN BAHARUDDIN (Technical IT Supervisor)
DR. ANIS SYAMIMI BINTI MOHAMED (Research Officer NODiP)
CIK NURUL IZZAH BINTI KAMARUDIN (Research Assistant NODiP)
PUAN ATHIRAH BINTI SHUHAIMI (Research Assistant NODiP)